
Do our patient's need fixing? Or do they need a bigger cup?
Audience: Therapists and people in pain
Blog Style: Lots of questions to consider
To help me understand pain and injuries and to hopefully help people I need to simplify things. One of the simplest ways to view pain is with the cup metaphor. It certainly has flaws but it does help look at the "big picture" of treatment. The cup metaphor suggests that pain occurs when all of the stressors/loads in our lives exceed the space in our cup. When we overflow we have pain.
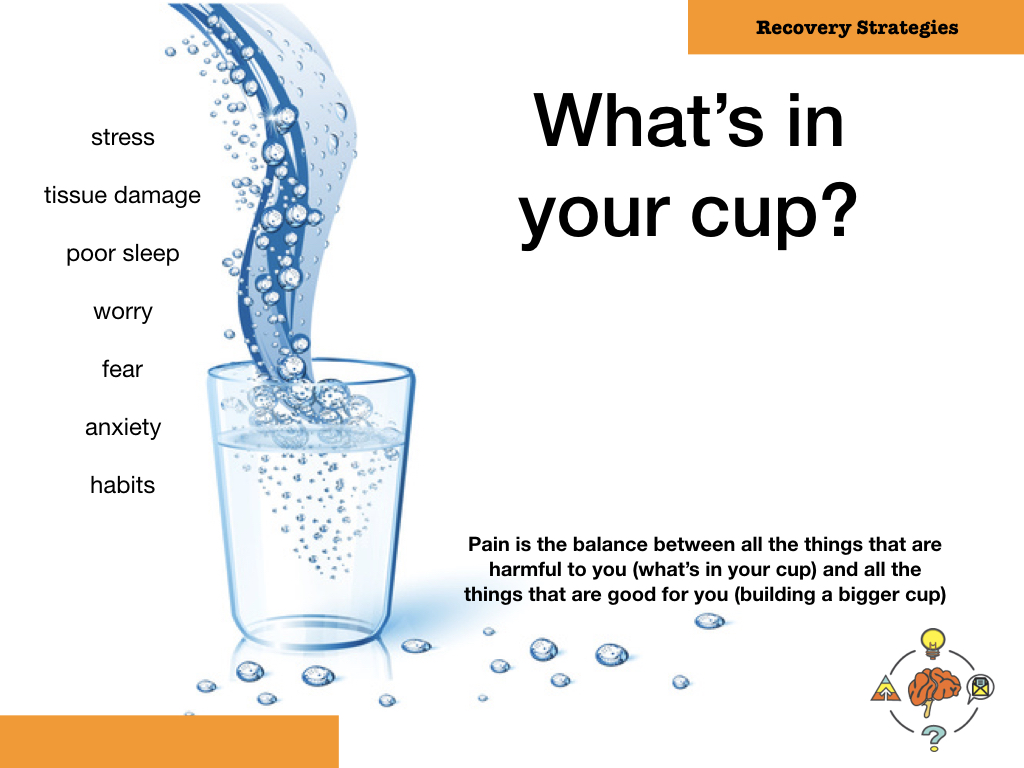
Its an actionable analogy because it says we can help in two ways:
1. Decrease some of stressors and loads that are in the cup
2. Build a bigger cup
The cup analogy is essentially saying that we have pain when we don't adapt positively to stressors in our life. It also recognizes that stressors are more than just the physical loads you put your body through. Its more than just some degenerative changes that you find on an x-ray (more on that here). Its more than how much you have to lift or bend. It also recognizes that other stressors like anxiety, fear, depression, catastrophizing, poor sleep, past history, family, work etc can all be in your cup. Please see the free book Recovery Strategies for ways to determine what might be in your cup.
Those stressors are not inherently bad. In fact, its those stressors in our life that catalyze a reaction in us. Its those stressors that can build us up, to tolerate more, to cope better and build RESILIENCY. Its like the old saying "if you want to get something done, you give it to a busy person".
A question to ponder...is there ever some factor related to pain that must be fixed? I often start my course with this question and what is amazing is how few conditions or pain contributors seemingly must be fixed.
For example, do we we fix or MUST we fix the following biomechancal variables often considered to be linked with pain.
Do you fix these?
I would argue that you don't have to fix these things. That they can exist and be associated with pain but following treatment the pain can be gone, function resolved and yet those things still exist. And this is the idea that we are building a bigger cup and learning to tolerate what is in the cup. Some related blog topics are here and here
The same with PsychoSocial Influences
Its the same with catastrophizing, beliefs about a weak core, rumination, anxiety and depression. All of these things can be linked with pain and might be contributing to the problem. But they don't all need to be fixed.
We can tolerate
We can adapt.
AS with everything we should challenge our biases
Just because we might not HAVE to change the stressors in our life because its possible to adapt to them I still think its worth trying to work on them. Because the difficulty with pain and almost everything is that we never know for sure what has to change and what is relevant.
So a great clinical question to ask yourself is:
Is there ever anything specific that must be done?
or
Is there ever some specific thing that must be addressed?
The questions are similar but different. One says that there is only 1 or 2 ways to address a problem and the other says there is definitely a contributor to pain that must be addressed to allow all the other good stuff to occur. Let me give two examples:
1. Your patient has an achilles tendinopathy. I would argue that you probably have to decrease some of their training loads, add some SPECIFIC load to the achilles to cause it to adapt to build up its tolerance to activity and slowly build up their training loads. In this case, I'm not sure you actually "fix" the tendinosis but you did need something pretty specific (achilles load) to prepare the person to tolerate that tendinosis
2. After listening and knowing your patient with low back pain you work together and decide that it could be helpful to start cycling, gardening and running again. All of this after a 2 year layoff. But you both realize that they have an incredible fear of reinjury, they are worried that their spine shouldn't be stressed and they are quite sure that the disc will get damaged with any of those activities that they used to do and that they want to resume. Just doing the cycling, gardening and running could work. But perhaps addressing those beliefs about reinjury and reconceptualizing how they view their spine must occur first or during the resumption of those meaningful activities. Here is an example where maybe the "fixing" is the addressing of the beliefs first before other aspects of treatment could be helpful.
Last, our next big question to improve our treatments is:
How do we build a bigger cup?
I cheat a little with this one. I assume the person I am working with has a lot of the answers. Once you have heard your patient's story, really understood it and then given them an explanation for what you think is contributing to their pain and how pain works (with respect to their specific story) we can ask our patient how they feel they could build a bigger cup. Of course, you should probably introduce the cup analogy first and then ask what they think can do to build their cup up. Its very similar to Kieran O'Sullivan asking "What is good for you?" or David Butler and Lorimer Moseley asking "What are your SIMs (Safety in Me)" in their great self help book The Protectometer?
You might also want to ask big questions like...
How can you be healthier?
How can I help you be healthier?
What I like about this "Calm Shit Down, Build Shit Back Up" approach is that it recognizes that there many ways to do this. I also think it is why we see clinical successes from therapists who seemingly practice very different from each other. With this view I get to keep taking different courses from different professionals to improve my ability to help people build a bigger cup. In summary, a nice slide of all the areas that you can build up is below. It shows part of a graphic from a great paper by the The top are the areas that could be addressed and improved to help with pain.
