
Janda's lower crossed syndrome has not been validated
Mike Reinold gets me thinking with much of his posts. He is someone I like discussing areas that we don't always agree on because he does it respectfully. He wrote about the lower crossed syndrome here about a recent study. Very briefly, the lower crossed syndrome suggests that tight hip flexors are associated with weak gluteus maximus muscles, weak abdominal muscles, tight erectors spine/hamstrings and lead to anterior pelvic tilt. This study looked at the relationship between hip extension mobility and gluteus maximus activity.
A related study is an old one that looked pelvic tilt, lordosis and abdominal performance. Guess what? No relationship. Kind of a knock against the idea that the anterior pelvic tilt of the lower cross syndrome is related to abdominal strength (paper here). These findings were also repeated in a study here.
That recent study looked at Gluteal activity during kettlebell swings. They also looked at hip flexor "tightness" as measured during the Modified Thomas Test. The authors did good work on this paper and kept their conclusions reasonable. But what will ultimately happen is that we will run a bit too far with what the study provides in our clinical interpretation. For one, this paper does not prove or even support Janda's lower crossed syndrome where it is suggested that "tight" hip flexors inhibit the Gluteus Maximus muscle via reciprocal inhibition. I'll try to lay out my reasoning for this below. But first the paper...
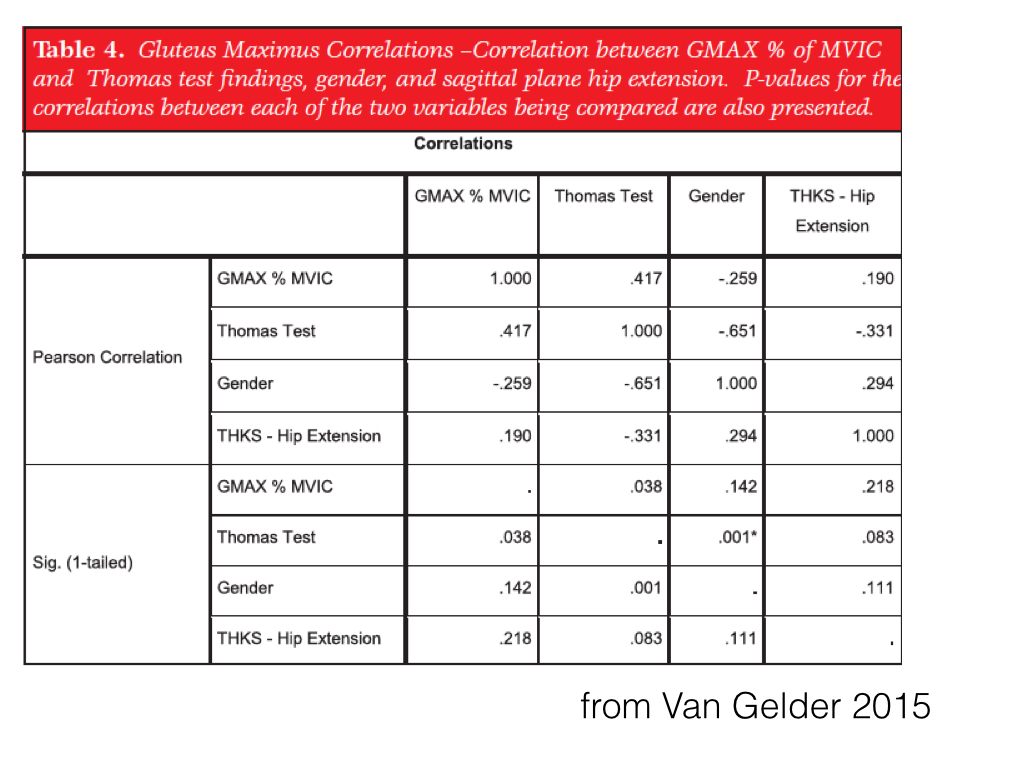
The authors concluded "During the THKS, a moderate positive correlation was found between average peak GMAX percent of MVIC and Thomas test measurements, with a correlation coefficient of 0.417."
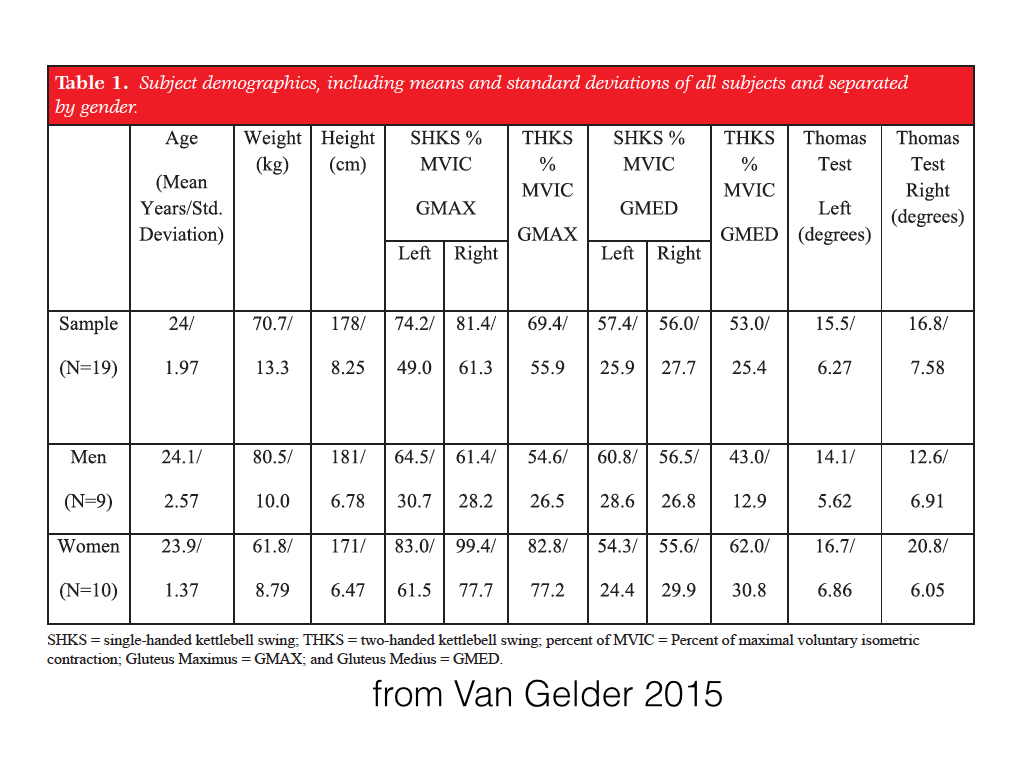
Below are the muscle activation numbers:
And below are the correlation co-efficients looking at GMax activity and what it is correlated to:
A few points to consider:
1. They write that hip flexor length is correlated to Gmax activity during the Two Handed KettleBell Swing with an r=.417.
This is not a strong correlation and may be spurious.
1a. Not really knock but it is interesting - they didn't report how GlutMax activity was correlated with hip flexor length during the single hand Kettlebell swing. Why not? Were these related? 2. An example of a spurious correlation would be that GMed activation is also related to hip flexor length with an r =.396. Why shouldn't we focus on this? Because it doesn't fit with the narrative. Would anyone argue that reciprocal inhibition is somehow working to inhibit the GMed from the hip flexors. They aren't agonists-antagonists. Makes no sense. Just a fluke. (again, not a fault of the researchers, just how when we interpret we may not consider everything).
3. Massive variability in the data. You'll notice that women had peak GMax EMG greater than 80%MVC while the men had EMG around 60% with huge variability. Does this mean that all the men had inhibited Glutes compared to the women. NO - again, there are other interpretations.
Percentage EMG is calculated with a numerator (the activity found during the Kettlebell swing) and the denominator (the activity found during the max contraction). The women were just functioning at a higher percentage of their maximum contraction.
But notice that the women had higher levels of hip extension during the Thomas Test.
You could completely re-intrepret this data and argue it differently.
One could argue that the peak activity found during the women's maximum contraction (the denominator) was low and therefore "inhibited". Thus they had a greater percentage during the Kettlebell swing because they were "weak" during the maximum test.
You can spin this stuff either way. You could argue that increased hip extensibility was related to decreased activity during the max contraction therefore the people were weaker and had to work harder during the KettleBell Swing because they had "loose" hip flexors. This is wrong but goes to show how these types of studies (through no fault of the authors) can't shed insight into these ideas.
3a. Combining the women with the men probably skewed the correlation data. Its not unsurprising that the women had a greater hip extension and its not unsurprising that the women had greater GMax EMG during the Kettlebell swing since it is likely that they would be weaker during hip extension. This kind of sets up that there will be trend to see more Glute Activity with more hip extension when you pool the sexes. I would be curious if you ran these correlations while separating the sexes what you would get. Probably an even weaker correlation. 4. The correlation was pretty weak and can be explained a number of different ways. We should also notice that the correlations between the GluteMax activity during a single hand KB swing and hip flexibility was reported.I am saying it again because people will keep saying that this study proves the lower crossed syndrome. It doesn't. But it doesn't disprove it either.
5. If the hips flexors are truly tight wouldn't you have to have more EMG activity to "power through" their resistance during hip extension. Probably not, but again this points out how biomechanical reasoning can justify different things.
6. None of these people had "tight hips" or at least not by the definition the authors gave. The authors argued a limitation in hip extensibility was when the Thomas test showed hip flexion of 10 degrees. All of them had hip extension where the thigh went below parallel. Where do you draw the line of what tight is? At what level of "tight" do the hip flexors start inhibiting the glutes if this actually happens.
If you just keep stretching and stretching the hip flexors will you keep getting more and more Glut activity? This reasoning doesn't make sense.
7. Why would the hip flexors inhibit the glutes during an activity that primarily sees the hip in a flexed position? The hip flexors aren't even being tensed - they are shortened. They aren't even turning on during this activity.
Final Caveats
I am not knocking this study. I think there is a lot of value you in it and I know they put a lot of work in it. I am only saying we should be cautious in how we interpret the researchers results. There is still a possibility that tight hip flexors actually do correlate with inhibited glutes. But this study doesn't support that. Maybe we need to compare a ground with VERY restricted hip extension versus another group. This paper tried to do this. And interestingly there study didn't support the lower crossed syndrome either.
Quick explanation of the Mills Paper mentioned 1 inch above
Why I say that this paper doesn't support the idea that tight hips negatively influence hip extensor function is because you only see a decrease in the activity of the GluteMax without a statistically significant increase in the activity of the hamstrings yet there is the same amount of hip extensor torque. If you have the same hip extensor torque and less GlutMax activity, without another muscle stepping in to help, you can say that the demands of the task have been met. You don't need any more GlutMax activity...maybe you are even more efficient - again, there are always other ways to view these things. See the chart below. And ignore the ratios. When you are dealing with numbers that small the ratios get amplified with tiny changes. Where my assessment might be wrong is that perhaps there was more Adductor Magnus activity to help out the Biceps Femoris. And to complicate things even more, was do "tight" hip flexors on reciprocally inhibited one of their antagonists (the GlutMax)? Aren't the hamstrings also antagonistic to the hip flexors?
